Dear Mr Brine,
I noted the Health and Social Care Committee’s inquiry, ‘Assisted dying/assisted suicide’ and wanted to highlight analysis the Office for National Statistics (ONS) published in April 2022, ‘Suicides among people diagnosed with severe or life-threatening conditions, England, 2017 to 2020’. This analysis looked at the risk of suicide in people with severe health conditions.
In April 2021, then-Secretary of State for Health and Social Care Matt Hancock MP wrote to the National Statistician expressing concerns about a lack of data on suicides where the person had been diagnosed with a terminal illness. He asked if the ONS would publish the appropriate data. The ONS agreed to assess the possibility of completing such analysis and to work with colleagues in the Department for Health and Social Care to do so.
ONS mortality records do not include medical conditions on the death certificate. However, the development of the Public Health Data Asset (PDHA), which links mortality records to the 2011 Census and Hospital Episode Statistics (HES), allows us to analyse wider medical circumstances of individuals before death. The study population consisted of all persons, alive on 1 January 2017, who were resident in England, and enumerated at the 2011 Census. People who travelled abroad for the purpose of assisted suicide would not appear as having died in our data.
We used HES records to identify individuals that were diagnosed or receiving first treatment for the following three health conditions:
- Low-survival cancer;
- Chronic Obstructive Pulmonary Disease (COPD);
- and Chronic ischemia.
These health conditions were chosen as in most cases patients with these conditions have a progressive condition which cannot be reversed by treatment and there is a substantial risk of death in those who are diagnosed. In many instances, people diagnosed with these conditions would meet the definition of having a terminal illness.
Our primary outcome was time to death due to suicide from the date of diagnosis which was restricted to between 1 January 2017 and 31 March 2020. The rate of suicide for patients with these conditions were then compared to rates for matched controls who were not diagnosed with these conditions. For each health condition, patients were matched on socio-demographic factors to ensure a reliable comparison.
There were 17,195 people who died due to suicide in the study period (1 January 2017 to 31 March 2020). Of these deaths, 455 (2.6%) were in patients diagnosed with COPD, 465 (2.7%) in patients with chronic ischemic heart conditions, and 58 (0.3%) were suicides in low survival cancer patients.
A diagnosis or first treatment for the selected health conditions is associated with an elevated rate of death due to suicide when compared with study participants with similar socio-demographic characteristics; participants known as matched controls. Matching is performed to assess whether the rate of suicide in people diagnosed with severe health conditions differs from that of people with a similar socio-demographic profile but not diagnosed with a severe condition.
Figure 1 shows that one year after diagnosis for low survival cancers, the suicide rate for patients (22.2 deaths per 100,000 people) was 2.4 times higher than the suicide rate for the matched controls (9.1 deaths per 100,000 people).
Figure 1: Suicide rate per 100,000 people, comparing patients who were diagnosed with severe health conditions with matched controls who have similar socio-demographic characteristics as patients but were not diagnosed with severe health conditions, England, Hospital Episode Statistics diagnosis, and deaths occurred between 1 January 2017 and 31 March 2020[1],[2]
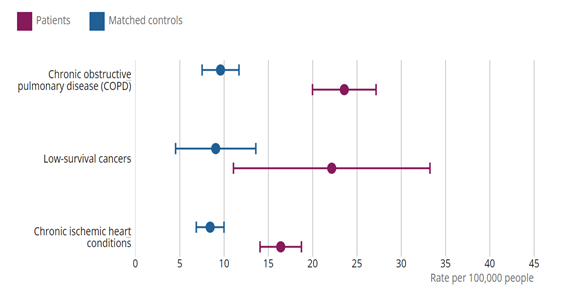
Source: Office for National Statistics – Public Health Data Asset For a more accessible version, please visit our accessibility policy.
Source: Office for National Statistics – Public Health Data Asset
One year after diagnosis for COPD, the suicide rate for patients (23.6 deaths per 100,000 people) was 2.4 times higher than the suicide rate for the matched controls (9.7 deaths per 100,000 people).
One year after diagnosis for chronic ischemic heart conditions, the suicide rate for patients (16.4 deaths per 100,000 people) was nearly two times higher than the suicide rate for the matched controls (8.5 deaths per 100,000 people).
Regarding people who travel abroad for an assisted death, unfortunately the ONS does not have access to any directly relevant data. Deaths of residents or citizens which occur abroad are recorded in line with the law of the country concerned and are not required to be registered in England and Wales under current legislation. Although a death abroad can be registered by the Foreign, Commonwealth and Development Office (FCDO) this process is voluntary, covers only a proportion of the deaths taking place abroad, and does not result in a civil registration available to the ONS for statistical analysis. There is therefore a gap in the international availability of official data concerning such deaths. The ONS will continue to engage with other national statistics institutes to examine how this data gap can be add addressed.
We continue to engage with stakeholders to understand demand for similar analysis in the future. We will keep you updated of any progress, and any future publications will be announced on the ONS release calendar
Please let us know if you would like to discuss any of this further.
Yours sincerely,
Emma Rourke
[1] Figures are for persons aged 10 years and over.
[2] The 95% confidence intervals are measures of the statistical precision of an estimate and show the range of uncertainty around the estimated figure.